Anaplastic large cell lymphoma
Anaplastic large cell lymphoma
Updated: 08/20/2024
© Jun Wang, MD, PhD
General features
- Moderately aggressive
- Likely in young population, men
- Both nodal and extranodal involvement
- Most common extranodal sites include skin, bone
- Morphologically similar to Hodgkin lymphoma
Key pathogenesis
- Translocation involving ALK (anaplastic lymphoma receptor tyrosine kinase)
- Abnormal activation of MAPK pathway
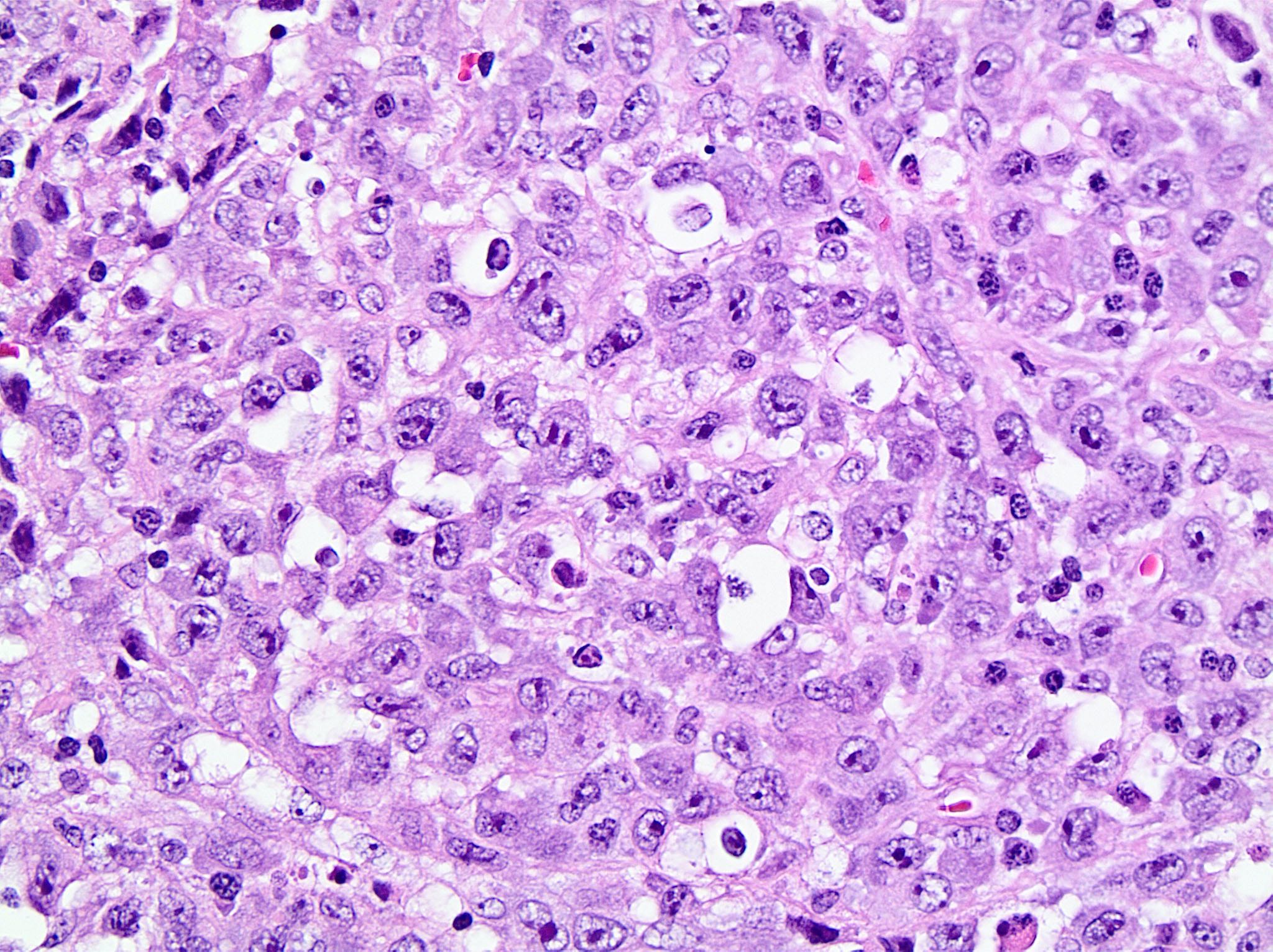
Key morphological features
- Markedly pleomorphic bizarre nuclei: Horseshoe ("hallmark") cells, wreath-like or multiple nuclei, multiple nucleoli, perinuclear eosinophilic region, occasional nuclear pseudoinclusions ("doughnut" cells)
{kind=link}
Markers
- Positive: CD30, ALK, T-cell markers such as CD5, CD45 (A marker negative in classic type Hodgkin lymphoma)
- Negative: B cell markers, such as CD20
Genetic abnormalities
- Translocation involving ALK gene
- T cell receptor (TCR) gene rearrangement
ALK- anaplastic large cell lymphoma
- T cell neoplasm with bizarre nuclei but ALK negative
- More common in 40 - 65 years, slightly more common in male
- Probably originates from activated T cells
- Commonly loss of CD3 and other T cell markers
- Gains of the 1q41-qter and 6p21 common
- Other molecular abnormalities include: rearrangement involving IRF4 or TP63, and activating mutations of STAT3
- Morphologically identical with ALK positive ALCL
- Positive for CD30, CD45
- Negative for ALK, EBV
- Chemotherapy with CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone) or CHOP plus etoposide (CHOEP)
Back to contents
Comments
Post a Comment