Mycosis fungoides
Mycosis fungoides
Updated: 06/16/2025
© Jun Wang, MD, PhD
General features
- Most common type of cutaneous T cell lymphoma
- More commonly seen in adults/elderly, men, African
- Unknown etiology
- Clonal CD4+ T cells
- Diagnosis based on clinical presentations, biopsy, molecular testing and immunopathologic profiling
Clinical presentations
- Four stages: Patch, plaque, tumoral and Sézary syndrome
- Patch stage: Pruritic erythematous macules or patches with telangiectasia and atrophy, may disappear spontaneously
- Plaque stage: Pruritic thichened plaques, may resemble psoriasis
- Tumoral stage: Tumor formation, either from plaques or de novo, may ulcerate
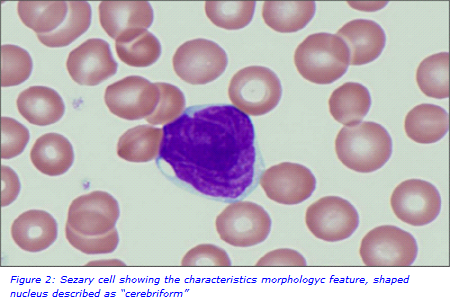
- Sézary syndrome
- Commonly erythroderma (80% of total body surface), may be scaly
- Lymphadenopathy
- Sézary cells in skin, lymph nodes and peripheral blood
- Usually do not evolve from patches, plaques or tumors
- May have marrow involvement
- WBC count might be normal or slightly elevated
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Key morphological features
- Patch stage: Psoriasiform changes, but intraepidermal clonal CD4+ T cells
- Plaque stage: Dermal infiltrate of atypical T cells with cerebriform nuclei alone or clustered in epidermis and in small sheets in dermis
- Tumoral stage: Dense dermal infiltrates of atypical T cells with cerebriform nuclei
- Sézary syndrome: More monotonous infiltrates, tumor cells in peripheral blood
{kind=link}
Markers
- Positive: CD4
- Negative: CD8
Other laboratory tests
- T-cell receptor gene rearrangement
- T-cell receptor gene sequencing
- Flow cytometry (SS): CD4+CD7- T cell subset
- Early stage: Topical corticosteroids, chemotherapy, retinoids, radiation, phototherapy, etc
- Advanced stages (IIB to IV): Local radiation, total skin electron beam therapy, systemic chemotherapy, phototherapy, interferon, retinoids, etc
Back to skin
tumors
Back to skin
pathology
Back to lymphoid neoplasms
Back to contents
Comments
Post a Comment