Autosomal Dominant Polycystic Kidney Disease
Autosomal Dominant (Adult) Polycystic Kidney Disease
Updated:10/05/2020
© Jun Wang, MD, PhD
General features
- Multisystemic and progressive disorder
- Most common inherited kidney disease
- Other organs involvement (eg, liver, pancreas, spleen)
- Third most common cause of end-stage renal disease
- Many patients require renal replacement therapy
Key pathogenesis
- Abnormal intracellular signaling by stimulation of cilia
- Abnormal tubule proliferation
Clinical features
- Pain: Abdomen, flank, or back, most common initial complaint
- Hematuria: Usually self-limited
- Hypertension: Very common, rise in diastolic blood pressure, tend to be more severe at early phase, but less problematic as renal insufficiency progresses
- Palpable, bilateral flank masses
- Presentations associated with renal failure
- Cystic masses in other organs, such as liver, pancreas, etc
- Causes of death
Most common: cardiac hypertrophy/coronary
artery disease
Neurologic events: ruptured intracranial
aneurysm or hypertensive intracerebral hemorrhage
Infections
Pathological findings
- Large kidney
- Cystic changes in all parts of nephron
- Cystic changes in other organs
- Cysts lined by cuboidal or flattened epithelium
- Scattered atrophic/compressed but still functional glomeruli
- Interstitial fibrosis and chronic inflammation
- Liver cysts lined by benign biliary epithelium
Genetic abnormalities
- Polycystin 1 (PKD1, chromosome 16p, most common)
- Polycystin 2 (PKD2, chromosome 4q)
Diagnosis
- Sonography
- CT, MRI
- Genetic testing
Additional workup
- Screening for intracranial aneurysm
- Glomerular filtration rate
Risk factors of progression
- PKD1 genotype
- Large kidneys
- Episodes of gross hematuria/frequent kidney infections
- Hypertension
- Multiple pregnancies
- African American
- Male
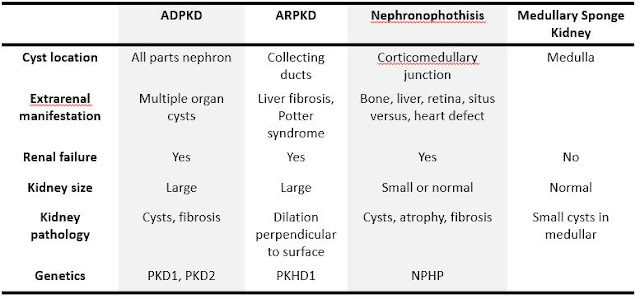
Differential diagnosis
Treatment

Treatment
- Pharmacologic therapy: Control blood pressure, renal failure, urinary tract infection, etc.
- Surgery: Drainage
- Transplantation: Kidney, liver
Back to kidney
masses
Back to contents
Comments
Post a Comment