Achalasia
Achalasia
Updated: 02/12/2021
© Jun Wang, MD, PhD
General features
- Lack of progressive peristalsis and partial/incomplete relaxation of lower esophageal sphincter (LES)
- Preferentially involves circular layer of muscularis propria, which is hypertrophied
- Markedly higher risk for squamous cell carcinoma
- Higher risk for aspiration, Barrett's esophagus, Candida infection, gastroesophageal reflux, lower esophageal diverticula, peptic ulceration, stricture
Etiology
- Primary: T cell mediated destruction or complete absence of myenteric ganglion cells in lower third of esophagus
- Secondary: Allgrove‘s syndrome, amyloidosis, Chagas' disease, diabetic autonomic neuropathy, polio, sarcoidosis, surgical ablation of dorsal motor nuclei, thyroid disease, tumor
Clinical presentations
- Dysphagia (most common), regurgitation, chest pain, heartburn, weight loss
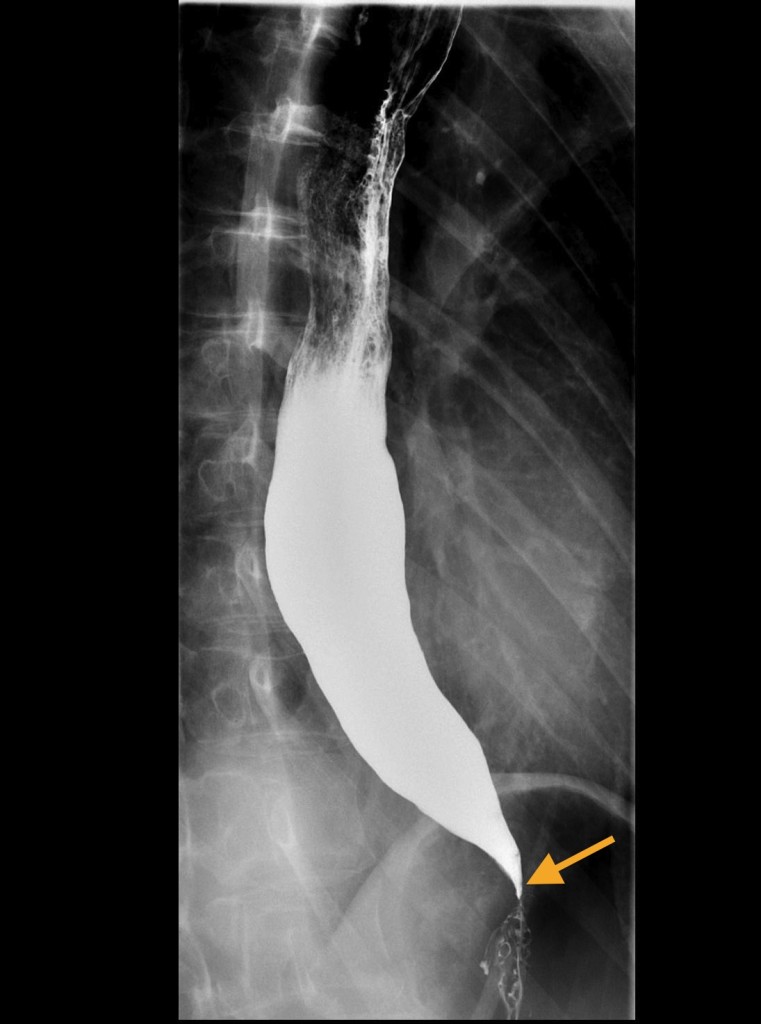
Diagnosis
- Barium swallow: Bird’s beak appearance, esophageal dilatation
- Esophageal manometry (standard criterion)
{kind=link}
Treatment
- Goal of therapy: Relieve symptoms
- Pharmacologic and other nonsurgical treatments: Calcium channel blockers, nitrates; endoscopic intrasphincteric injection of botulinum toxin
- Surgical treatment: Laparoscopic Heller myotomy; peroral endoscopic myotomy
- If surgery fails: Endoscopic dilatation
- Esophagectomy: Last resort
Back to contents
Comments
Post a Comment