Erythema multiforme
Erythema multiforme, Steven Johnson Syndrome/Toxic Epidermal Necrosis
Updated: 10/10/2025
© Jun Wang, MD, PhD
General features
- Uncommon, acute process
- May be self limited in minor forms, or life threatening
- Risk factors: Immune abnormalities, including HIV infection, corticosteroid exposure, bone marrow transplant, autoimmune disorders, and inflammatory bowel disease
- Likely EM and SJS/TEN are two different diseases
- EM: slightly more common in young male
- SJS/TEN: more common in female
- Diagnosed based on clinical presentations
Pathogenesis
- Type IV hypersensitivity reaction associated with infections, drugs, carcinoma / lymphoma, or collagen vascular disorders
- Immune complex mediated reaction in some cases
- Erythema multiforme minor and major: more commonly associated with viral infections
- SJS/TEN: more commonly associated with drug reaction
Classifications
- Erythema multiforme minor: Typical targets or raised, edematous papules distributed acrally
- Erythema multiforme major: Typical targets or raised, edematous papules distributed acrally with involvement of one or more mucous membranes; epidermal detachment involves less than 10% of total body surface area (TBSA).
- SJS/TEN: Widespread blisters predominant on the trunk and face, presenting with erythematous macules and one or more mucous membrane erosions
{kind=link}
{kind=link}
{kind=link}
Steven-Johnson syndrome: < 10% Epidermal detachment
Toxic epidermal necrolysis: > 30% Epidermal
detachment
{kind=link}
Overlapping SJS/TEN: 10-30%
epidermal detachment
Clinical features
- Affects skin (distal extremities, palms, soles) and mucous membranes
- Variable (multiform) lesions – papules, macules, vesicles, bullae, target
- Either localized (erythema multiforme minor) to systemic, life-threatening (Stevens-Johnson syndrome/Toxic epidermal necrolysis)
- Starting from extremities symmetrically with centripetal spreading
- Pruritus usually absent
- Target lesion:
{kind=link}
Central dark area or a blister
surrounded by
A pale edematous zone surrounded
by
A peripheral rim of erythema
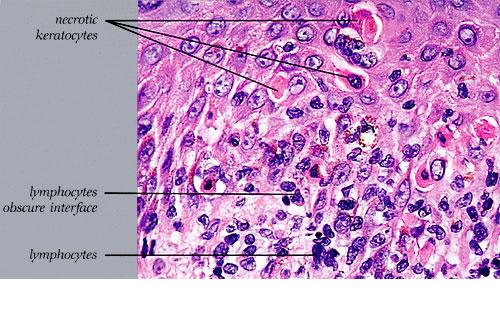
Pathological findings
- Lichenoid infiltrate
- Keratinocytic necrosis
- Vascular damage
{kind=link}
{kind=link}
Stevens-Johnson
syndrome and toxic epidermal necrolysis
- May be life threatening
- Wide spread erythematous macules and targetoid lesions
- Mucous membranes commonly involved
- Likely immune-complex mediated
- Full thickness epidermal necrosis with minimal dermal inflammation
- Diagnosis
- History of drug exposure or febrile illness
- Prodrome of acute onset febrile illness and malaise
- Rapidly progressing painful rash
- Erythematous macules, targetoid lesions with two zones of color, diffuse erythema to blisters
- Mucosa involvement
- Necrosis and sloughing of epidermis
- Treated symptomatically
- Pay special attention to airway and hemodynamic stability, fluid status, wound/burn care, and pain control
- Extensive debridement of nonviable epidermis followed by immediate cover with biologic dressings
{kind=link}
Management
- Symptomatic treatment, including oral antihistamine, local skin care, etc
- Transfer to and care in a burn unit for patients with Stenvens-Johnson Syndrome and toxic epidermal necrolysis
- Identify the cause if possible
Prognosis
- Most are self-limited
- Mortality proportional to the total body surface area of sloughed epithelium
- Skin lesion usually heal with hyper and/or hypopigmentation
- Scarring rare unless infected secondarily
Back to contents
Comments
Post a Comment