Lichen planus
Lichen planus
Updated: 12/18/2023
© Jun Wang, MD, PhD
General features
- Likely immune disorder
- More common in 30-60
- May be confined to oral mucosa
- Usually regressin 6 to 18 months
Pathogenesis
- Cell-mediated (CD8+ T cells) immune response to antigens at basal cells or dermoepidermal junction, with unknown triggering factors
- May be associated with immunity disorders, such as ulcerative colitis, dermatomyositis, etc, and certain infections, such as hepatitis C
- Stressful events may play a role in the onset or exacerbation
Clinical features
- Initially on flexural skin of limbs, then spread after a week
- May involve mucosa
- 6 Ps (Pruritic,Polygonal, Planar, Purple, Papules, Plaques)
- Various subtypes including
Follicular: Lichenplanopilaris, hair follicles centered
Hypertrophic:
Extremely pruritic, more common on extensor
surfaces of lower extremities
{kind=link}
Vesicular/bullous
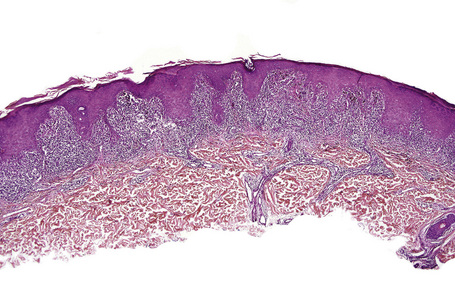
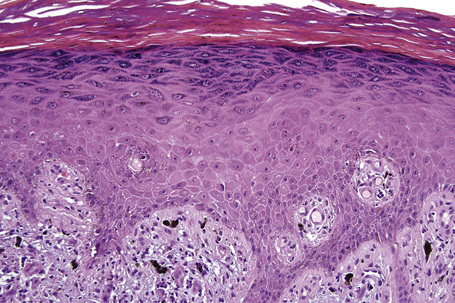
Pathological features
- Lichenoid inflammation: Band like chronic inflammatory infiltrate (T cells and macrophages) that destroys the dermoepidermal junction
- Hyperkeratosis and acanthosis with prominent granular cell layer
- Sawtoothing of rete pegs
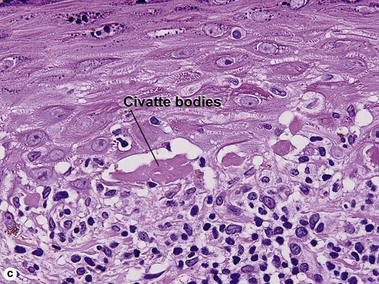
- Civatte bodies (apoptotic basal cells, PAS+)
- Artifactual cleft formation at dermal epidermal junction
- Occasional subepidermal bullae (Bullous lichen planus)
{kind=link}
{kind=link}
{kind=link}
Immunofluorescence studies
- Clumped deposits of IgM in lichen planus, Civette bodies
- May be IgG, IgA, complements, fibrinogen, but less common
Diagnosis
- Commonly based on clinical findings
- Biopsy (deep enough to include dermoepidermal junction) if uncertain
- Individualized treatment
- Steroids, tropical or systemic, metronidazole, retinoids, etc.
- UV-B radiation or psoralen with UV-A radiation for widespread cases
- Usually self-limited
Back to contents
Comments
Post a Comment