Prostatic adenocarcinoma
Prostatic adenocarcinoma
Updated: 01/29/2021
© Jun Wang, MD, PhD
General features
- Predominantly acinar type, less commonly ductal type
- Most common non cutaneous cancer in men in the United States
- Predominantly > 50
- More common in North America, Australia and northern and central Europe
Risk Factors
- Genetic factors
Ashkenazi Jewish ancestry
BRCA1, BRCA2, Lynch syndrome
CHEK, ATM, HOXB13, etc
- Environmental factors
High animal fat diet
Cigarette smoking
Obesity, etc
- Hormones and growth factors
Androgen
Insulin and insulin-like growth factor
- Protective factors
Lycopenes
Coffee
Soy products
Vitamin D, etc
- Hormones, especially androgens and androgen receptor signaling
Amplification/overexpression:
Most common
Mutation: Commonly
in castrate-resistant cancers, most are gain-of-function mutation
Splice variants:
Active AR splice variants (SVs), created by gene splicing or genomic
rearrangement
Posttranslational
modifications: Phosphorylation, methylation, etc
Intratumoral
androgen synthesis
Clinical features
- Asymptomatic or nonspecific presentations
- Urinary complaints or retention, back pain, hematuria, etc
- Symptoms associated with metastasis
Screening approaches
- Serum prostate specific antigen (PSA)
- Digital rectal exam
- Biopsy if abnormal PSA, or rectal exam
Pathological findings
- More common in posterior portion
- More common from peripheral zone (posterior and lateral)
- Firm mass, usually invisible
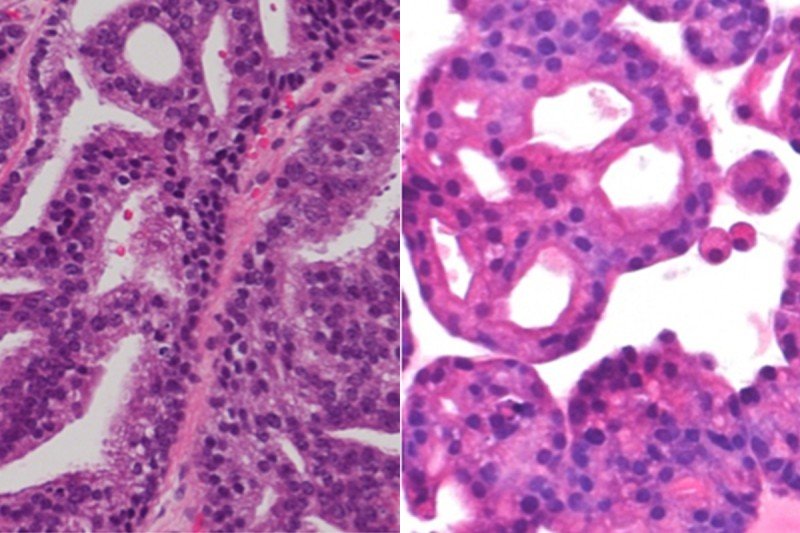
- Predominantly acinar type, a small portion may be ductal type
- Small glands, tubular or cribriform types
- Single layer, NO basal layer
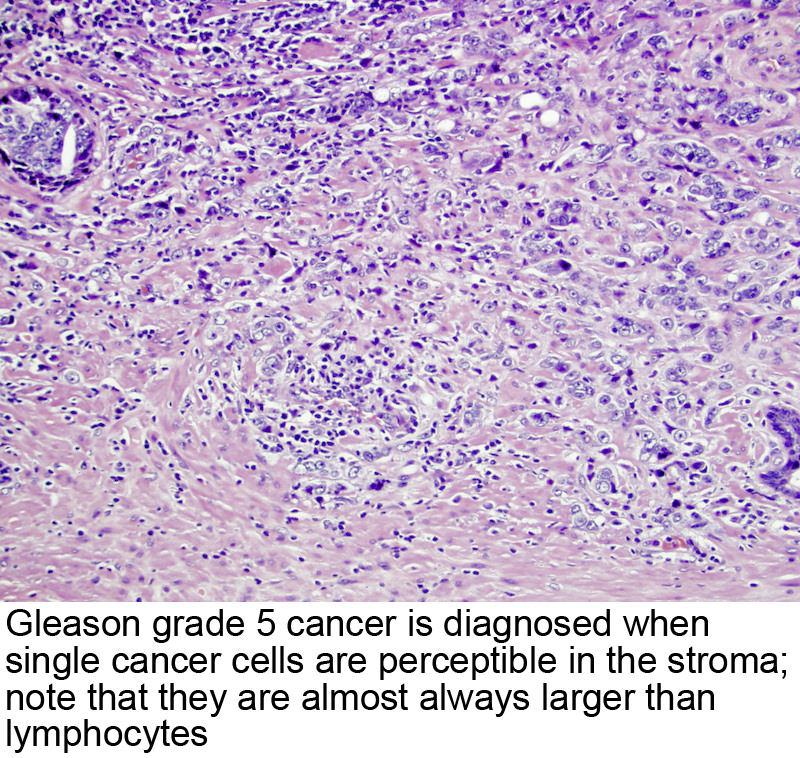
- Solid cords if high grade
- Graded based on glandular differentiation: Gleason score
- Vascular and perineural invasion not uncommon
{kind=link}
{kind=link}
Marker
- Positive: Racemase, PSA
- Absence of basal layer: NO reactivity to p63 and 34betaE12
Management
- Localized tumor
Radical
prostatectomy
Radiation therapy
Androgen
deprevation therapy
Active
surveillance
- Metastatic cancer:
Rarely curable
with current technology
Therapy focus on
symptom relief and slow disease progression
- Prognostic factors: Staging, Gleason grade, tumor volume, capsular status, etc
Back to contents
Comments
Post a Comment