Prostatic nodular hyperplasia
Benign prostatic hyperplasia
Updated: 01/03/2025
© Jun Wang, MD, PhD
General features
- AKA benign prostatic hypertrophy (BPH)
- Incidence increases with age
- Considered a normal part of the aging process in men
- Hormonally dependent on testosterone and dihydrotestosterone production
- Periurethral (transitional zone) nodules likely compress urethra and cause obstructive symptoms
- May cause urinary retention, renal insufficiency, recurrent urinary tract infections, gross hematuria, and bladder calculi
Pathogenesis
- Activation of androgen receptor
- Stromal type II 5-alpha-reductase convert testosterone to dihydrotestosterone (DHT)
- DHT promotes glandular and stromal hyperplasia
- Estrogen may increase quantity of androgen receptor
- Other growth factors
Clinical features
- Due to chronic bladder outlet obstruction
- Urinary frequency
- Urinary urgency
- Hesitancy: Difficulty initiating the urinary stream; interrupted, weak stream
- Incomplete bladder emptying - The feeling of persistent residual urine, regardless of the frequency of urination
- Straining - The need strain or push (Valsalva maneuver) to initiate and maintain urination in order to more fully evacuate the bladder
- Decreased force of stream - The subjective loss of force of the urinary stream over time
- Dribbling - The loss of small amounts of urine due to a poor urinary stream
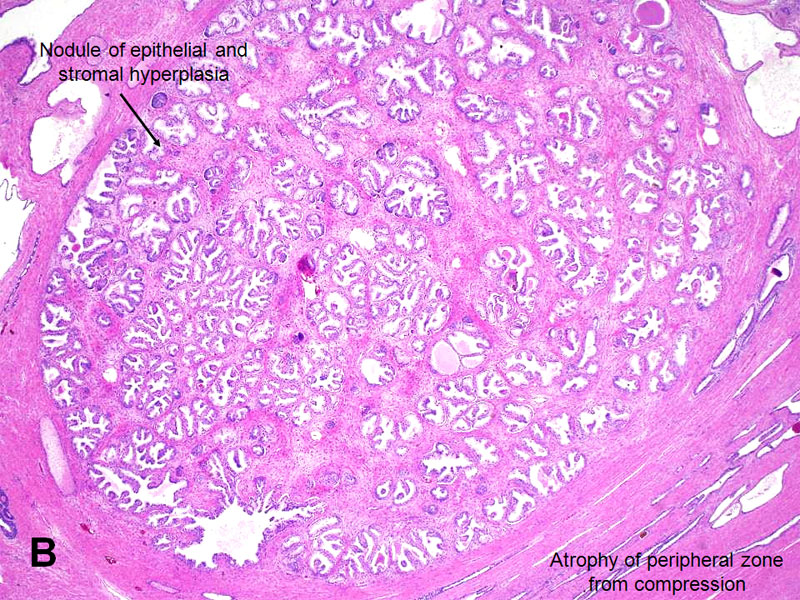
Pathological findings
- Enlarged prostate with nodular appearance
- Trabeculation of bladder due to chronic obstruction
- Benign hyperplasia of glands and stroma
- Usually more prominent of glandular components
- Two layers of glandular cells, luminal and basal
- NO atypia
- Intact basal layers: highlighted by p63, high molecular keratin (34betaE12)
- No correlation between histology and symptoms
{kind=link}
{kind=link}
Marker
- Negative for racemase
Management
- Surgery
Transurethral resection of prostate (TURP)
Suprapubic prostatectomy
- Androgen antagonists, smooth muscle relaxers (5 alpha reductase inhibitors decrease DHT and in many cases, prostatic volume and symptoms), minimally invasive treatment (i.e. ethanol ablation in Europe)
Back to pathology of male reproductive system
Back to contents
Comments
Post a Comment