Sexually transmitted penile infections
Sexually transmitted penile infections
Updated: 08/13/2025
© Jun Wang, MD, PhD
Syphilitic chancre
- Caused by Treponema pallidum
- Presentation of primary syphilis
- Usually solitary
- Painless hard chancre
- Commonly at inner foreskin, coronal sulcus, penile shaft and penile base
- Pathological features
Same for syphilitic chancre at any location
Spirochetes
identified by silver stain (Warthin-Starry’s statin)
- Laboratory test
- Screening tests:
- Detect anti-cardiolipin antibodies in patient with syphilis
- Rapid plasma reagin (RPR)
- Venereal Disease Research Laboratory (VDRL)
- Toluidine Red Unheated Serum Test (TRUST)
- Confirmatory tests
- May be used as initial tests due to automation
- Fluorescent treponemal antibody-absorption (FTA-ABS)
- Microhemagglutination test for antibodies to T.
pallidum (MHA-TP)
- T. pallidum particle agglutination assay (TPPA)
- T. pallidum enzyme immunoassay (TP-EIA)
- Chemiluminescence immunoassay (CIA)
- Treatment: Penicillin
Chancroid
- Etiology: Gram-negative rod Haemophilus ducreyi
- Painful genital ulcer and inguinal adenopathy
- Mainly in developing countries, particularly Africa, Asia and Latin America
- Cofactor for HIV transmission
- Zonation of ulcer
Upper layer: Ulcer base with fibrin,
neutrophils and necrosis
Middle layer: Granulation tissue, palisading
vessels and thrombosis
Deep layer: Marked lymphoplasmacytic infiltrate
- Microbiology: Chains of Gram negative rods
- Evaluation of other causes of genital ulcer, such as syphilus, Herpes
- Diagnosis: Confirmed by culture or PCR to identify H. ducreyi
- Treatment: Antibiotics (Azithromycin, Ceftriaxone, or erythromycin)
Herpes
- Most common cause of genital ulceration
- Usually caused by DNA viruses herpes simplex virus 2 (HSV2) and less commonly HSV1
- Spreads by direct contact with lesions
- May spreads by asymptomatic shedding when no lesion is apparent
- More common in genital area and mouth
- Clusters of small papules and macules, followed by vesicles that rupture and cause painful ulcers
- Pathological features
Multinucleation, molding, margining of chromatin,
same as skin
herpes
Background of acute inflammation
- Treatment: Antiviral drugs
Granuloma inguinale
- Caused by Klebsiella granulomatis, a gram negative rod
- More common in African American, lower social-economic status
- Endemic in tropical and subtropical climates such as Papua New Guinea, parts of South Africa, parts of India, Indonesia and Australian aborigines
- More common in foreskin, glans, penile shaft or scrotum
- Four cutaneous presentations
- Nodular: Initially a small pruritic erythematous nodule at infection site that ulcerates; may have satellite lesions
- Ulcerovegetative: Painless beefy red ulcer with distinct raised border
- Cicatricial: Cicatricial plaques
- Hypertrophic/verrucous: vegetating mass similar to wart
- Pathological features
{kind=link}
Large mononuclear cells with Donovan bodies (large intracytoplasmic encapsulated bipolar bodies)
Background plasma cell and neutrophil infiltrate
- Diagnosis: Histology or cytology (crush) prep of tissue from ulcer edge to identify Donovan bodies
- Treatment: Antibiotics (erythromycin, tetracyclin, ampicillin etc)
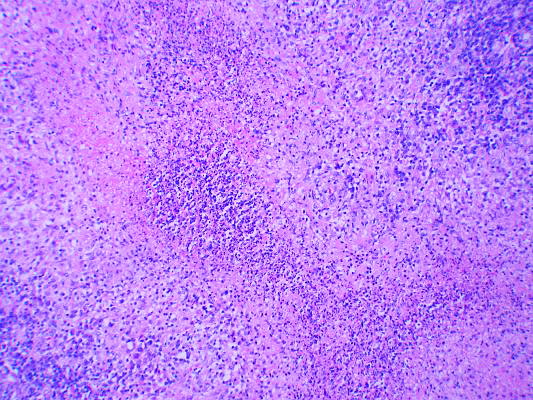
Lymphogranuloma venereum
- Caused by Chlamydia trachomatis
- Incidence highest in the tropics and subtropics
- Causes either inguinal, rectal or rarely pharyngeal syndrome
- Incubation period: 3-12 days
- Initial lesion: Painless ulcer at inoculation site appears and rapidly disappears
- Inguinal syndrome: Enlarged superficial and deep inguinal lymph nodes (groove sign) with suppurative granulomatous changes, with focal necrosis (stellate abscesses)
- Diagnosis: Clinical presentations with molecular tests (Nucleic Acid Amplification Testing), serology
- Treatment: Tetracycline (except during pregnancy) or erythromycin
{kind=link}
Condyloma acuminatum
- Human papillomavirus-related
- Transmitted through skin contact during sex
- Most commonly affects young males in teens and 20’s
- Many HPV infections don’t lead to condyloma
- Rarely transform into malignancy
- Pathologic features
- Treatment: Cryotherapy, laser, curettage, excision, etc
Back to contents
Comments
Post a Comment