Waterhouse Frederichsen syndrome
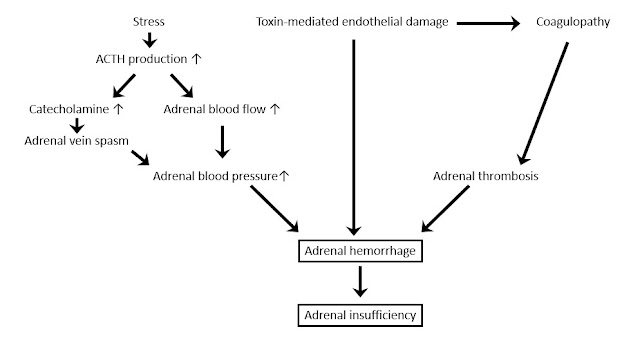
Waterhouse Frederichsen syndrome Updated: 06/21/2022 © Jun Wang, MD, PhD General features Adrenal insufficiency Due to bilateral/unilateral adrenal hemorrhage Associated with bacterial or viral infection Commonly associated with meningococcal infection Other associated pathogens include Haemophilus influenzae Pseudomonas aeruginosa Escherichia coli Streptococcus pneumoniae Pathogenesis Clinical presentations Sudden onset Nonspecific presentations: headache, fever, weakness, abdominal/flank pain, anorexia, etc Signs of shock : Tachycardia, hypotension, etc Abdominal rigidity or rebound tenderness If associated with meningococcemia: petechial rash , purpura fulminans, other neurological abnormalities Key Laboratory findings Features of Disseminated intravascular coagulation Leukocytosis Hyponatremia and hyperkalemia: Mineralocorticoid deficiency Hypoglycemia: glucocorticoid deficiency Elevated : ACTH, renin Decreased : Aldosterone...
