Bullous pemphigoid
Bullous pemphigoid
Updated: 02/09/2021
© Jun Wang, MD, PhD
General features
- Subepidermal, nonacantholytic, autoimmune disease
- More common in elder population
- Most patients need long term treatment
Pathogenesis
- IgG antibodies to hemidesmosomal proteins BP230 (BPAG1) and BP180 (BPAG 2)
Clinical features
- Large tense pruritic skin blisters
- Rarely involves oral or ocular mucosa
- Bullae don't rupture easily, and heal without scarring unless infected
- High level IgG1 and IgG4 against BP180 (BPAG 2) 16A domain indicate worse prognosis
- Acute or subacute
- Widespread tense skin blisters, frequently pruritic
- Subepidermal blister
- May have eosinophilic infiltrate
{kind=link}
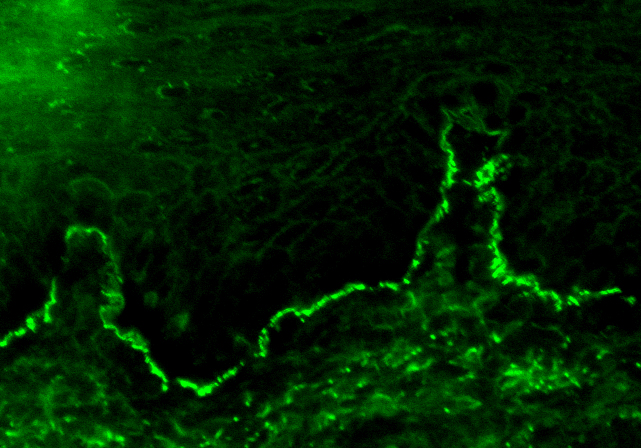
Immunofluorescence feature
- IgG along dermoepidermal junctions
{kind=link}
Management
- Corticosteroid
- Immunosuppressant
- Treatment of infection
Back to contents
Comments
Post a Comment