Pemphigus
Pemphigus
Updated: 02/09/2021
© Jun Wang, MD, PhD
General features
- Rare, nonhereditary, chronic, autoimmune disease
- Ages 30-59; no gender preference
- May be associated with internal malignancies, including thymoma
- Intraepidermal blisters with acantholysis
- Benign, but may be fatal if untreated in extreme cases
Pathogenesis
- Autoantibody against desmoglein 1 and 3 (desmosome components)
Pemphigus
vulgaris
- Most common type
- May involve both skin and oral mucosa
- Superficial vesicles, easily ruptured with painful erosion
- Healing usually accompanied by post-inflammatory hyperpigmentation
- Deaths may occur due to staphylococcal infection, or pulmonary embolism
- Suprabasilar bullae with single row of basal cells resides on basement membrane
{kind=link}
{kind=link}
Pemphigus
foliaceus
- Endemic in Brazil and Columbia, but may be sporadic in the world
- Often involving skin of trunk
- Mucosa NOT involved
- Crusts and shallow erosions on healthy skin with blisters formed after rubbing
- Mild clinical behavior
- Vesicles at the granular layer with mild inflammation
{kind=link}
- Senear–Usher syndrome
- Usually middle age adults
- Localized area, resemble lupus malar rash on face
- May be considered as a localized less severe form of pemphigus foliaceus
.%20Practicall%20skills%20of%20history%20taking.%20Assesment-1..files/image031.jpg){kind=link}
Pemphigus
vegetans
- Rare
- Considered a localized form of pemphigus vulgaris
- Verrucous plaques in affected regions
- Oral cavity commonly affected
- Subtle supra basal acantholysis with epidermal hyperplasia, intraepidermal eosinophilic and neutrophilic microabscesses
{kind=link}
Pemphigus
paraneoplastic
- Associated with internal tumor
- Involving both oral mucosa and skin
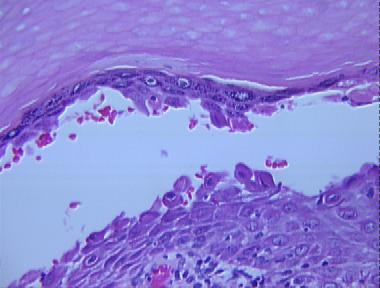
Pathological features
- Intraepidermal vesicles
- Acantholysis
- May have eosinophilic infiltrate
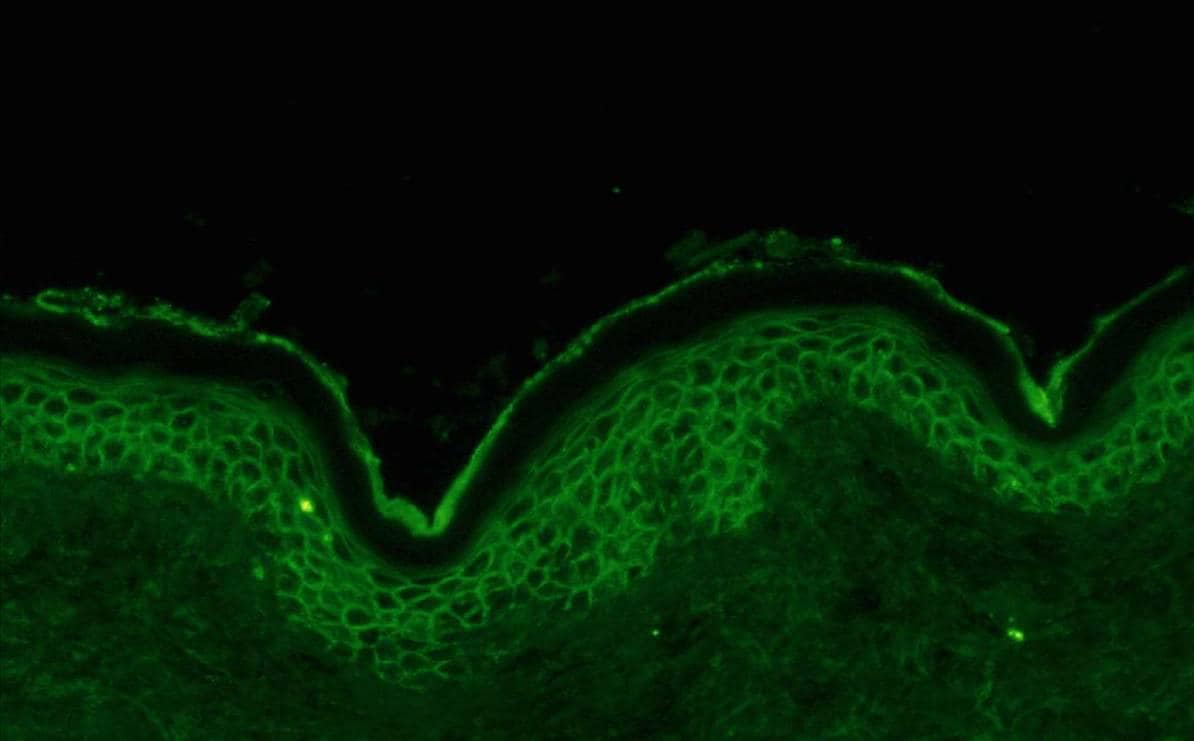
Immunofluorescence feature
- IgG along intercellular junctions within epidermis
{kind=link}
Management
- Corticosteroid
- Immunosuppressant
- Wound care, etc
Back to contents
Comments
Post a Comment