Sialadenitis
Sialadenitis
Updated: 07/24/2023
© Jun Wang, MD, PhD
General features
- Infection/inflammation of salivary glands
Etiology
- Variable etiology including infection, autoimmune reaction or trauma
Bacterial sialadenitis
- Rare
- Usually due to ascending bacterial infection of ductal system
- Unilateral painful enlargement of salivary gland
- Usually clinical diagnosis
- May cause abscess requiring surgical drainage
Viral sialadenitis
- Mumps is the most common type
- Other associated viruses: cytomegalovirus, coxsackievirus, herpes, etc
- Tender enlargement of affected salivary gland
- Usually clinical diagnosis
- Supported by serology or RT-PCR testing
- Mumps
- Most common in pts < 15 years
- Commonly bilateral parotid glands
- May cause epididymo-orchitis
Chronic sialadenitis and sialolithiasis
- AKA obstructive sialadenitis
- Due to impedance of saliva flow resulted from stone formation
- More common in male
- More common in submandibular gland
- May be associated with increased calcium content in secretions
- Presentation: Intermittent periprandial pain, single gland swelling
- Diagnosis: clinical or sialography
- Heterogeneous group
- Predominantly involving parotid, followed by submandibular gland
- Swelling of affected glands, with or without pain
- May be associated with obstruction (with atrophy and fibrosis), rheumatoid arthritis (older women), Sjogren syndrome, sialolithiasis, mumps
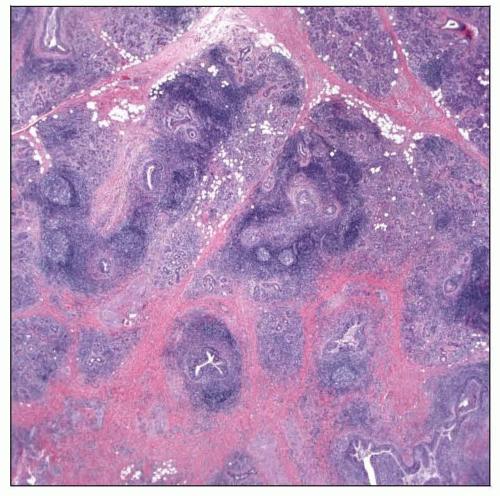
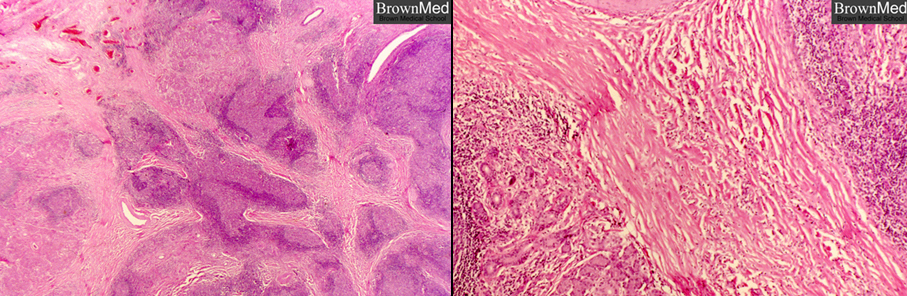
- Pathological features
{kind=link}
{kind=link}
IgG4 related dacryoadenitis and sialadenitis
- Old term: Mikulicz disease/syndrome
- Spectrum of IgG4
related sclerosing diseases, including autoimmune pancreatitis
- Involving lacrimal and salivary glands
- More common in submandibular glands
- Usually present as a mass (Küttner tumor or sclerosing sialadenitis if submandibular)
- Serum IgG4 concentration elevated, but may be normal
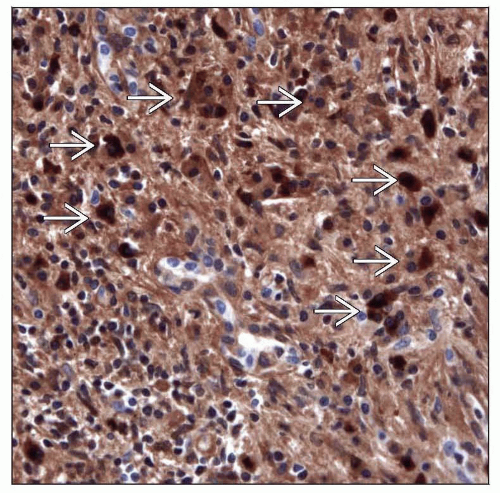
- Diagnosis based on histologic feature, elevated IgG4/IgG ratio
- Three major pathological features
Dense
lymphoplasmacytic infiltrate with IgG4+ plasma cells and CD4+ cytotoxic T cells
{kind=link}
{kind=link}
{kind=link}
Back to contents
Comments
Post a Comment