Practice questions vesiculobullous disorders
Practice questions
Vesiculobullous disorders
Updated: 03/01/2019
© Jun Wang, MD, PhD
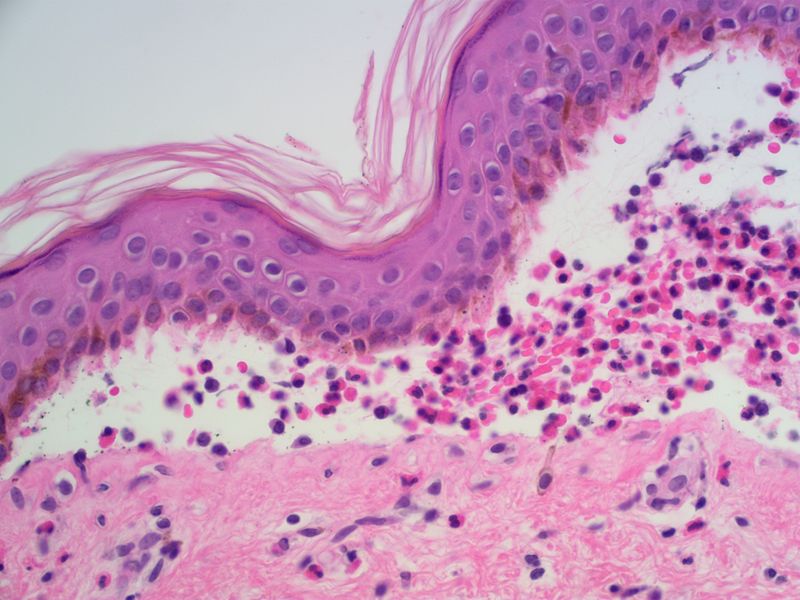
1. Use this
image and this case for the next four question. A 44-year-old man presents
with painful blistering lesions involving his chest, back and oral mucosa.
These blisters start from his oral mucosa and spread to his chest and back. His
past medical history is unremarkable. Physical examination reveals blisters
from a few millimeters to 5 cm in greatest dimension. Some have ruptures with
purulent exudates. An image of the biopsy is shown. Detached clusters of round
to polygonal keratinocytes are seen. There is no evidence of significant
cytological atypia. What is the diagnosis?

(Image credit: Nephron [CC BY-SA 3.0 (https:\creativecommons.org\licenses\by-sa\3.0)])
A. Bullous pemphigoid
B. Dermatitis herpetiformis
C. Epidermolysis bullosa
D. Herpes
E. Pemphigus vulgaris
2. A 44-year-old man presents with painful blistering
lesions involving his chest, back and oral mucosa. These blisters start from
his oral mucosa and spread to his chest and back. His past medical history is
unremarkable. Physical examination reveals blisters from a few millimeters to 5
cm in greatest dimension. Some have ruptures with purulent exudates. An image
of the biopsy is shown. Detached clusters of round to polygonal keratinocytes
are seen. There is no evidence of significant cytological atypia. What is directly
causing these changes?
(Image credit: Nephron [CC BY-SA 3.0 (https:\creativecommons.org\licenses\by-sa\3.0)])
A. Autoimmune process
B. Congenital defect
C. Trauma
D. UV light
E. Viral infection
3. A 44-year-old man presents with painful blistering
lesions involving his chest, back and oral mucosa. These blisters start from
his oral mucosa and spread to his chest and back. His past medical history is
unremarkable. Physical examination reveals blisters from a few millimeters to 5
cm in greatest dimension. Some have ruptures with purulent exudates. An image
of the biopsy is shown. Detached clusters of round to polygonal keratinocytes
are seen. There is no evidence of significant cytological atypia. What
immunofluoscence test results is most likely seen?
(Image credit: Nephron [CC BY-SA 3.0 (https:\creativecommons.org\licenses\by-sa\3.0)])
A. Clumped deposit of IgM at dermoepidermal junction
B. Deposit of IgG along epidermal intercellular
junctions
C. Granular deposit of IgA at dermal papillae
D. Linear deposit of IgG along dermoepidermal junction
4. A 44-year-old man presents with painful blistering
lesions involving his chest, back and oral mucosa. These blisters start from
his oral mucosa and spread to his chest and back. His past medical history is
unremarkable. Physical examination reveals blisters from a few millimeters to 5
cm in greatest dimension. Some have ruptures with purulent exudates. An image
of the biopsy is shown. Detached clusters of round to polygonal keratinocytes
are seen. There is no evidence of significant cytological atypia. Abnormality
of what molecule is most likely associated with these findings?
(Image credit: Nephron [CC BY-SA 3.0 (https:\creativecommons.org\licenses\by-sa\3.0)])
A. BP180
B. Collagen VII
C. Desmoglein 1
D. Keratin 5
E. Laminin 5
5. A 55-year-old woman presents with erosions on her
chest and back for 4 months. She has a history of type 2 diabetes, but denies
any history of allergy. Physical examinations reveals small erosions up to 1.5
cm with an erythematous base, located on her trunk. No other abnormalities are
noted. Biopsy reveals skin with mild spongiosis. Intraepidermal vesicles are
noted at the granular layer. There is no significant acanthosis, hyperplasia or
cytological atypia. Immunofluorescence studies reveal deposit of IgG along
keratinocytic borders. What is the diagnosis?
A. Bullous pemphigoid
B. Epidermolysis bullosa
C. Pemphigus erythematosus
D. Pemphigus foliaceus
E. Pemphigus vegetans
6. Use this
case for the next 2 cases. A 79-year-old man presents with thickened skin
at his arms. The lesions developed from clusters of small pustules. He has a
history of type 2 diabetes and hypertension. His family history is significant
for skin cancers. Physical examination reveals rubbery grayish plaques at both
arms. A few pustules are noted in adjacent skin. Biopsy of the lesions reveals
marked acanthosis, focal spongiosis and intraepidermal microabscesses. No
significant cytological atypia is noted. Immunofluorescent studies reveal
diffuse IgG deposit along keratinocyte borders. What is the diagnosis?
A. Bullous pemphigoid
B. Pemphigus erythematosus
C. Pemphigus foliaceus
D. Pemphigus vegetans
E. Squamous cell carcinoma
7. A 79-year-old man presents with thickened skin at
his arms. The lesions developed from clusters of small pustules. He has a
history of type 2 diabetes and hypertension. His family history is significant
for skin cancers. Physical examination reveals rubbery grayish plaques at both
arms. A few pustules are noted in adjacent skin. Biopsy of the lesions reveals
marked acanthosis, focal spongiosis and intraepidermal microabscesses. No
significant cytological atypia is noted. Immunofluorescent studies reveal
diffuse IgG deposit along keratinocyte borders. What is likely the cause of
these findings?
A. Autoimmune antibody against desmoglein 1
B. Complement deposit at dermoepidermal junction
C. Congenital defect of keratin 5
D. UV-induced malignant transformation of
keratinocytes
E. Viral infection
8. Use this
image and this case for the next four question. A 65-year-old man presents
with large blisters at his left shoulder and chest for a month. His past
medical history is unremarkable. These blisters appear to be tense and contain
clear fluid. An image of the biopsy is shown. There is no evidence of significant
cytological atypia. What is the diagnosis?
(Image credit: Sarahkayb [CC
BY-SA 4.0 (https:\creativecommons.org\licenses\by-sa\4.0)])
A. Bullous pemphigoid
B. Dermatitis herpetiformis
C. Epidermolysis bullosa
D. Herpes
E. Pemphigus vulgaris
9. A 65-year-old man presents with large blisters at
his left shoulder and chest for a month. His past medical history is
unremarkable. These blisters appear to be tense and contain clear fluid. An image
of the biopsy is shown. There is no evidence of significant cytological atypia.
What is the cause of these findings?
(Image credit: Sarahkayb [CC
BY-SA 4.0 (https:\creativecommons.org\licenses\by-sa\4.0)])
A. Autoimmune process
B. Congenital defect
C. Trauma
D. UV light
E. Viral infection
10. A 65-year-old man presents with large blisters at
his left shoulder and chest for a month. His past medical history is
unremarkable. These blisters appear to be tense and contain clear fluid. An
image of the biopsy is shown. There is no evidence of significant cytological
atypia. Abnormality of what molecule is most likely associated with these
findings?
(Image credit: Sarahkayb [CC
BY-SA 4.0 (https:\creativecommons.org\licenses\by-sa\4.0)])
A. BP180
B. Collagen VII
C. Desmoglein 1
D. Keratin 5
E. Laminin 5
11. A 65-year-old man presents with large blisters at
his left shoulder and chest for a month. His past medical history is
unremarkable. These blisters appear to be tense and contain clear fluid. An
image of the biopsy is shown. There is no evidence of significant cytological
atypia. What immunofluoscence test results is most likely seen?
(Image credit: Sarahkayb [CC
BY-SA 4.0 (https:\creativecommons.org\licenses\by-sa\4.0)])
A. Clumped deposit of IgM at dermoepidermal junction
B. Deposit of IgG along epidermal intercellular
junctions
C. Granular deposit of IgA at dermal papillae
D. Linear deposit of IgG along dermoepidermal
junction
12. Use this
case for the next 3 questions. A 12-year-old boy presents with pruritic
skin lesions at his back. He has a history of intermittent bloating and
diarrhea. He denies history of abdominal pain, cough, fever, and other
symptoms. Physical examination reveals small pustules in clusters at his back. No
other abnormalities are noted. Biopsy of the vesicle reveals separation along
dermoepidermal junction with neutrophilic aggregates. The keratinocytes have
mild atypia but no multinucleated cells nor nuclear abnormalities are seen. Special
stains reveals no evidence of microorganisms. What is most likely the
diagnosis?
A. Bullous pemphigoid
B. Dermatitis herpetiformis
C. Epidermolysis bullosa
D. Herpes
E. Pemphigus vulgaris
13. A 12-year-old boy presents with pruritic skin
lesions at his back. He has a history of intermittent bloating and diarrhea. He
denies history of abdominal pain, cough, fever, and other symptoms. Physical
examination reveals small pustules in clusters at his back. No other
abnormalities are noted. Biopsy of the vesicle reveals separation along
dermoepidermal junction with neutrophilic aggregates. The keratinocytes have
mild atypia but no multinucleated cells nor nuclear abnormalities are seen.
Special stains reveals no evidence of microorganisms. What pattern of
immunofluorescence study is expected?
A. Clumped deposit of IgM at dermoepidermal junction
B. Deposit of IgG along epidermal intercellular
junctions
C. Granular deposit of IgA at dermal papillae
D. Linear deposit of IgA along dermoepidermal junction
E. Linear deposit of IgG along dermoepidermal junction
14. A 12-year-old boy presents with pruritic skin
lesions at his back. He has a history of intermittent bloating and diarrhea. He
denies history of abdominal pain, cough, fever, and other symptoms. Physical
examination reveals small pustules in clusters at his back. No other
abnormalities are noted. Biopsy of the vesicle reveals separation along
dermoepidermal junction with neutrophilic aggregates. The keratinocytes have
mild atypia but no multinucleated cells nor nuclear abnormalities are seen.
Special stains reveals no evidence of microorganisms. What is most likely
associated with his bloating and diarrhea?
A. Absence of enteric ganglion
B. Autoimmune gastritis and duodenitis
C. Gluten hypersensitivity
D. Herpes gastritis
E. Pyloric smooth muscle hyperplasia
15. Use this
case for the next 3 questions. A 1-day-old boy develops skin sloughing and
appears to be in pain. New blisters and sloughing appear during the initial
management. The skin around joints is extremely easy to be peeled off. He was
born at term. The prenatal course is unremarkable. Biopsy reveals separation
between basal and upper layer epidermis. Both dermoepidermal junction and
dermis are morphologically unremarkable. There is no spongiosis, acantholysis,
nor inflammation. What is likely the diagnosis?
A. Bullous pemphigoid
B. Dermatitis herpetiformis
C. Epidermolysis bullosa simplex
D. Herpes
E. Pemphigus vulgaris
16. A 1-day-old boy develops skin sloughing and
appears to be in pain. New blisters and sloughing appear during the initial
management. The skin around joints is extremely easy to be peeled off. He was
born at term. The prenatal course is unremarkable. Biopsy reveals separation
between basal and upper layer epidermis. Both dermoepidermal junction and
dermis are morphologically unremarkable. There is no spongiosis, acantholysis,
nor inflammation. Defect of what molecule is likely to causing these
presentations?
A. BP180 or BP230
B. Collagen VII
C. Desmoglein 1 or desmoglein 3
D. Keratin 5
E. Laminin 5
17. A 1-day-old boy develops skin sloughing and appears
to be in pain. New blisters and sloughing appear during the initial management.
The skin around joints is extremely easy to be peeled off. He was born at term.
The prenatal course is unremarkable. Biopsy reveals separation between basal
and upper layer epidermis. Both dermoepidermal junction and dermis are
morphologically unremarkable. There is no spongiosis, acantholysis, nor
inflammation. What test is likely to confirm the diagnosis?
A. Gram stain and culture
B. Immunofluorescence mapping
C. Lymphocyte phenotyping
D. Quantitative serum immunoglobulin levels
E. Viral DNA analysis
18. Use this
image and this case for the next 2 questions. A 7-year-old boy presents
with deformation of feet. He has had painful skin erosions since birth. He has
a few family members with easy peeled skin. An image of his feet is shown. What
is likely the diagnosis?
(Image credit: Master Sgt. Keith A. Milks [Public
domain], via Wikimedia Commons [Public domain])
A. Bullous pemphigoid
B. Epidermolysis bullosa dystrophic type
C. Epidermolysis bullosa junctional type
D. Epidermolysis bullosa simplex
E. Kindler syndrome
19. A 7-year-old boy presents with deformation of
feet. He has had painful skin erosions since birth. He has a few family members
with easy peeled skin. An image of his feet is shown. What defect is likely to
be associated with these presentations?
(Image credit: Master Sgt. Keith A. Milks [Public
domain], via Wikimedia Commons [Public domain])
A. Actin-ECM linkage
B. Collagen VII
C. Desmoglein 1 or desmoglein 3
D. Keratin 5
E. Laminin 5
Back to vesiculobullous
disorders
Back to contents
Comments
Post a Comment