Gastric adenocarcinoma
Gastric adenocarcinoma
Updated: 11/03/2023
© Jun Wang, MD, PhD
General features
- Most common malignancy of stomach
- More common: Japan, Chile, Northern Italy, China, Portugal, Russia
- More common in men, elder, populations of low social economic status
- May be associated with Lynch Syndrome
Pathogenesis
- Intestinal type non-cardia gastric cancer: Helicobacter pylori infection, progressing from chronic non-atrophic gastritis to atrophic gastritis, then intestinal metaplasia, and finally dysplasia (Correa’s cascade), Wnt/beta-catenin pathways
- Cancer of cardia: Associated with Barrett esophagus, chronic GERD and obesity
- Diffuse type CA or Familial: CDH1 (E-cadherin) mutation
{kind=link}
Classification by morphology
- Tubular adenocarcinoma
- Papillary adenocarcinoma
- Mucinous adenocarcinoma, tumor shows >50% mucin
- Poorly cohesive carcinomas, including signet ring cell carcinoma
- Other rare variants: Adenosquamous carcinoma, etc
Intestinal
type
- Majority, associated with intestinal metaplasia
- Mean age 55 years, more common in men
- Risk factors: Diet containing nitrates, smoked and salted foods, pickled vegetables, lack of citrus fruit, lack of green leafy vegetable; also low socioeconomic status, cigarette smoking
- Host factors: chronic gastritis (intestinal metaplasia is a precursor lesion), H pylori infection, autoimmune gastritis, partial gastrectomy, gastric adenomas
Diffuse
type
- Also called linitis plastica or signet ring cell adenocarcinoma
- Aggressive clinical course
- Infiltrative growth of poorly differentiated discohesive malignant cells
- More common in younger age
- No known risk factors except rarely hereditary diffuse gastric cancer (rare, autosomal dominant, related to mutations in E-cadherin gene (CDH1)
Kruckenberg tumor
- Bilateral ovarian metastases
- Most often of gastric origin, may from other primary site
- Commonly composed of mucin-producing, signet-ring cancer cells
Clinical presentations
- Early stage usually asymptomatic
- Symptoms in later stage include: Indigestion, nausea or vomiting, dysphagia, GI bleeding, weight loss, etc
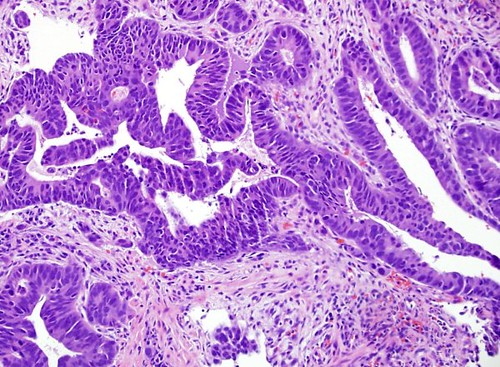
Key pathological features
- Atypical glandular cells, with or without glandular formation
- Intestinal type: bulky tumor, with or without ulcer, atypical tubular glands
- Diffuse type: Diffuse thickening of gastric wall, no discrete tumor, signet ring cells
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Genetic abnormalities
- Wnt/beta-cateninpathways: intestinal type
{kind=link}
Loss of function mutation of APC
Gain of function mutation of beta catenin
- E-cadherin gene (CDH1): diffuse type
Treatment
- Surgery, chemo, radiation
Poor prognostic indicators:
- Younger age
- Proximal half of stomach, deep invasion, infiltrative margin
- Diffuse histologic type
- Positive surgical margins (predicts local recurrence), lymph node metastases
Back to contents
Comments
Post a Comment