MUTYH-associated polyposis
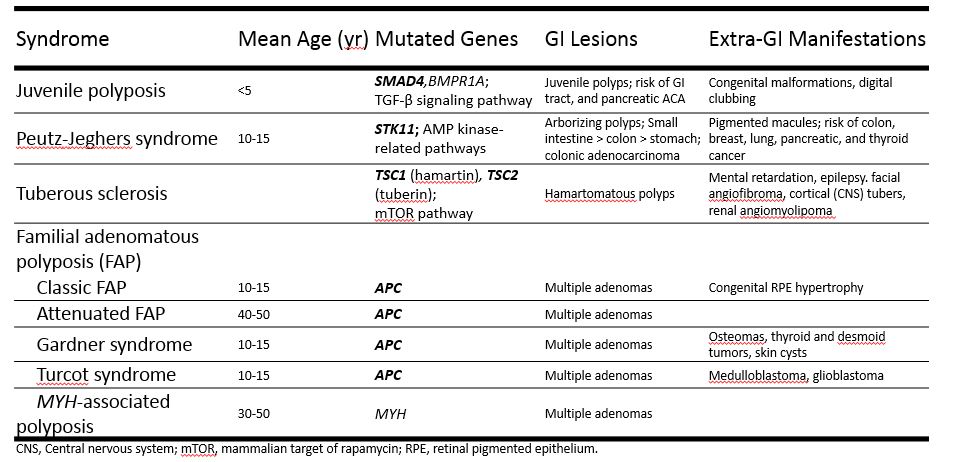
MUTYH-associated polyposis Updated: 03/02/2021 © Jun Wang, MD, PhD General features AKA MYH-associated polyposis Autosomal recessive Considered a mild form of familial adenomatous polyposis Biallelic mutation of MUTYH gene (DNA mismatch repair) Less 1% of patients with colorectal cancer Pathogenesis MUTYH mutation results in mutation of other genes , including APC and KRAS Clinical presentations Multiple colon polyps , usually less than 100, by age 50 to 60 Extracolonic presentations Polyps may be seen in other organs, such as stomach and small intestine Osteoma Sebaceous hyperplasia or adenoma , etc Pathological features Primarily adenoma Severe dysplasia at early age Genetic abnormalities MUTYH Diagnosis Suspicious presentations Cumulative 10 or more colorectal adenomas Colorectal adenoma with extracolic features of FAP Genetic testing for MYH Back to intestinal tumors Back to syndromes Back to contents