Practice question answers, skin tumors 1
Practice
question answers, skin tumors 1
© Jun Wang, MD, PhD
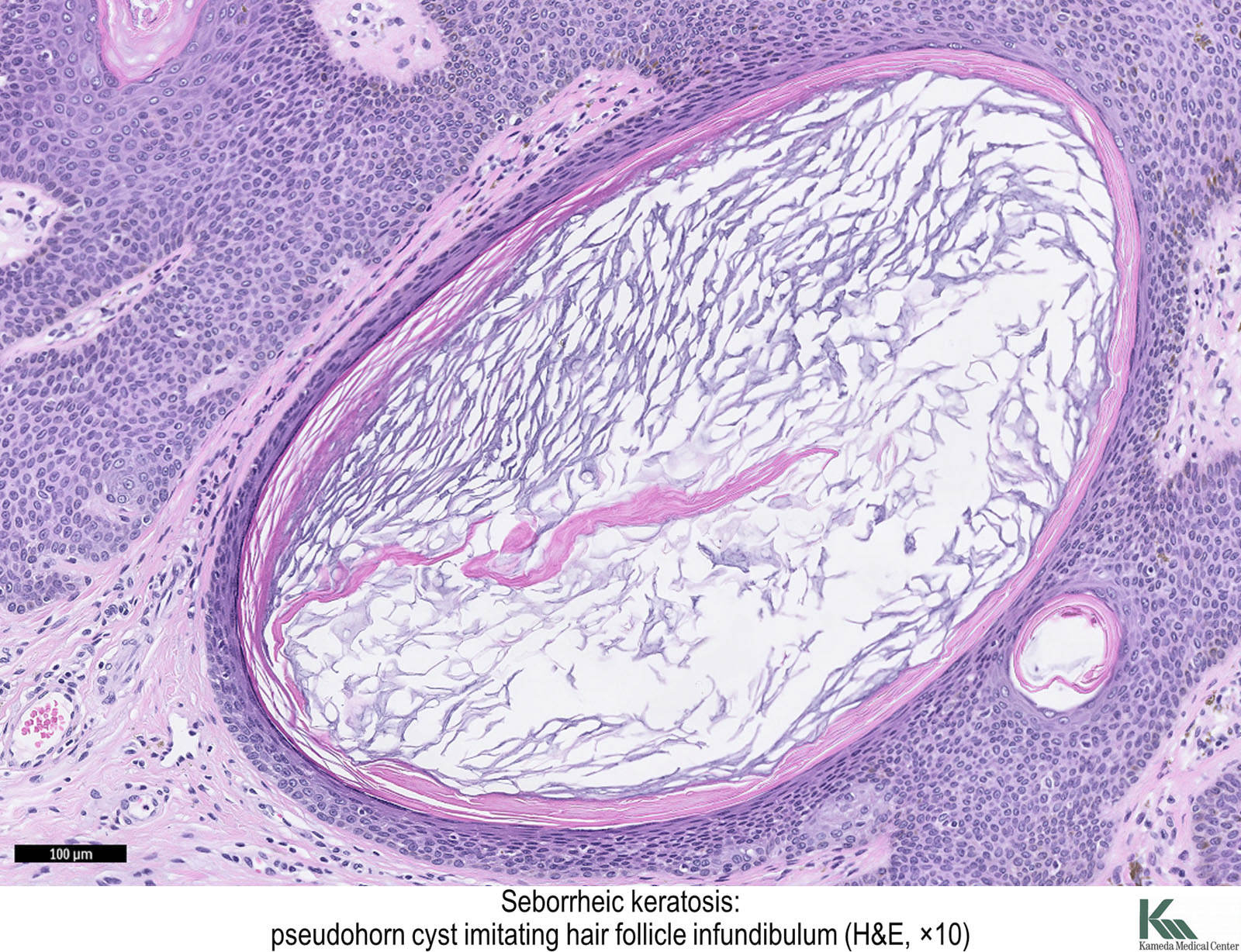
1. C. Epidermal proliferation with pseudohorn
cysts is most consistent with seborrheic
keratosis. Actinic
keratosis has dysplasia limited to basal layer, usually not epidermal
proliferation or pseudohorn cysts. Merkel
cell carcinoma has intradermal sheets of poorly differentiated cells with
scant cytoplasm and express neuroendocrine markers such as CD56, synaptophysin and
chromogranin. Squamous
cell carcinoma has irregular nests or cords of atypical squamous cells with
intercellular
bridges and/or keratin pearl formation. Verruca vulgaris is caused by human
papillomavirus and usually has koilocytes.
{kind=link}
2. B. The skin lesion has epidermal proliferation with
pseudohorn
cysts, most consistent with seborrheic
keratosis. Sudden increased number of seborrheic
keratosis is suggestive of Leser-Trelat
syndrome, associated with internal organ malignancies, especially GI tract.
This patient has clinical presentations of dysphagia and weight loss, with a
history of Barrett’s
esophagus, highly suspicious for esophageal
adenocarcinoma. Guttate
psoriasis is scaly dermatosis with psoriasiform epidermal hyperplasia. Neurofibromatosis
1 has multiple neurofibromas,
characterized by proliferation of spindle cell with slender nuclei, and
positive reactivity to S100. Nevoid basal cell carcinoma syndrome has basal
cell carcinoma. Sezary
syndrome has diffuse erythroderma, lymphadenopathy and CD4 positive
malignant Sezary cells in peripheral blood.
3. C. See discussion of question 2. Abnormal keratinocyte
turnover is seen in psoriasis.
Human papillomavirus may cause wart, and a small portion of squamous cell carcinoma
of skin. NF 1 mutation is seen in neurofibromatosis
1. UV light is the most important cause of skin cancers, including squamous
cell carcinoma, basal
cell carcinoma and melanoma.
4. C. Skin hyperpigmentation at folds with mildly
thickened skin is likely acanthosis
nigricans, a condition possibly associated with internal malignancies, or
insulin resistance. Acute bacterial infection or fungal infection usually has
erythematous changes, edema, and scaly surface. Melanocytic proliferation
usually has well demarcated borders. Metastatic cancer has mass formation.
5. A. Polypoid skin growth of with a fibrovascular
core covered by benign epidermis and lack adnexa is acrochordon.
Dermatofibroma
is a well defined intradermal spindle cell proliferation that is positive for
factor XIIIa and negative for CD34. Dermatofibrosarcoma
protuberans is an invasive hypercellular dermal spindle cell proliferation
with cytological atypia, and is positive for CD34 and negative for factor XIIIa.
Neurofibroma
has spindle cell with slender nuclei, and positive reactivity to S100. Schwannoma
has cellular
component(Antoni A) that palisades (Verocay bodies), and myxoid component
(Antoni B).
{kind=link}
6. B. Skin cyst with
greasy contents and lined by epidermis with granular layer is epidermal
cyst. Dermatophytosis
is fungal infection but not cyst formation. Pilar
cyst is lined by epidermal without granular layer and has packed solid
contents. Pilomatrixoma
is characterized by sheets of basaloid cells and ghost cells. Teratoma is germ
cell tumor with mature skin differentiation in other structures, such as ovary.
7. B. See discussion of question 6. Squamous
cell carcinoma has irregular nests or cords of atypical squamous cells with
intercellular
bridges and/or keratin pearl formation.
8. D. Well demarcated skin growth of small
keratinocytes connecting to epidermis is most consistent with eccrine
poroma. Actinic
keratosis has dysplasia limited to basal layer. Basal
cell carcinoma has irregular budding, nest, cords of basaloid cells with
scant cytoplasm with peripheral palisading. Cylindroma
has compact nests of basaloid cell forming a jigsaw puzzle pattern separated by
thick basement membrane. Squamous
cell carcinoma has irregular nests or cords of atypical squamous cells with
intercellular
bridges and/or keratin pearl formation.
9. B. See discussion of question 8. Syringoma
has benign small tadpole shaped glandular proliferation in a fibrotic
background.
10. C. Multiple cylindromas
with a positive family history are consistent with the familial form (turban
tumor syndrome, Brooke-Spiegler syndrome) that is associated with CYLD
mutation. Beta-catenin mutation can be seen in ovarian
endometrioid adenocarcinoma, stomach
cancer, colon adenoma,
solid-pseudopapillary
neoplasm and pilomatricoma.
BRAF mutation can be seen in various disorders, including melanocytic
nevus and melanoma.
MSH2 is a DNA mismatch repair gene and its mutation is seen in colon
cancer, Lynch
syndrome and its variant Muir-Torre
syndrome, etc. PTCH mutation is seen basal
cell carcinoma.
11. E. Syringoma
has benign small tadpole shaped glandular proliferation in a fibrotic
background. Cylindroma
has compact nests of basaloid cell forming a jigsaw puzzle pattern separated by
thick basement membrane. Eccrine
poroma has well demarcated skin growth of small keratinocytes connecting to
epidermis. Invasive
ductal carcinoma has irregular ducts lined by atypical cells. Sebaceous
adenoma has lobulated growth of generative cells (dark) and sebaceous cells
(light).
12. C. Sebaceous
adenoma has lobulated growth of generative cells (dark) and sebaceous cells
(light). When associated with presentation of Lynch
syndrome, as seen in this case as early onset of colon
cancer, and family history of associated malignancies, it is likely Muir-Torre
syndrome. Brooke-Spiegler syndrome is familial form of cylindromas.
Cowden syndrome has multiple tricholemmoma,
hamartomas and associated malignancies. Neurofibromatosis
2 has schwannoma,
meningiomas, café au lait, etc. Nevoid basal cell carcinoma syndrome has basal
cell carcinoma.
13. D. See discussion of question 10.
14. C. Pilomatrixoma
is characterized by sheets of basaloid cells and ghost cells. Cylindroma
has compact nests of basaloid cell forming a jigsaw puzzle pattern separated by
thick basement membrane. Pilar
cyst is lined by epidermal without granular layer and has packed solid
contents. Sebaceous
adenoma has lobulated growth of generative cells (dark) and sebaceous cells
(light). Syringoma
has benign small tadpole shaped glandular proliferation in a fibrotic
background.
15. E. Benign basaloid and squamous proliferation with
primitive hair follicle is consistent with trichoepithelioma.
Basal
cell carcinoma has irregular budding, nest, cords of basaloid cells with
scant cytoplasm with peripheral palisading. Cylindroma
has compact nests of basaloid cell forming a jigsaw puzzle pattern separated by
thick basement membrane. Epidermal
cyst has greasy contents and lined by epidermis with granular layer. Pilomatrixoma
is characterized by sheets of basaloid cells and ghost cells.
16. E. Lobular or plate-like growth of pale pink,
glassy cells with palisading at periphery is compatible with tricholemmoma.
Basal
cell carcinoma has irregular budding, nest, cords of basaloid cells with
scant cytoplasm with peripheral palisading. Cylindroma
has compact nests of basaloid cell forming a jigsaw puzzle pattern separated by
thick basement membrane. Trichoepithelioma
has benign basaloid and squamous proliferation with primitive hair follicle formation.
Eccrine
poroma has well demarcated skin growth of small keratinocytes connecting to
epidermis.
17. A. Well defined dermal spindle cell proliferation with
immunohistrochemistry profiles of positive factor XIIIa and negative CD34
expression is consistent with dermatofibroma.
Dermatofibrosarcoma
protuberans has invasion, and is positive for CD34 and negative for factor
XIIIa. Leiomyoma
is positive for desmin. Melanoma
and neurofibroma
are positive for S100.
18. B. See discussion of question 17.
19. D. Dermatofibrosarcoma
protuberans is associated with fusion of COL1A1 and PDGFB. Also see
discussion of question 10.
20. D. Spindle cell proliferation with slender nuclei
and positive reactivity to S100 is consistent with neurofibroma.
Dermatofibroma
is positive for factor XIIIa. Dermatofibrosarcoma
protuberans is positive for CD34. Leiomyoma
is positive for desmin. Skin tag is polypoid skin growth of with a
nonneoplastic fibrovascular core covered by benign epidermis and lack adnexa.
It is negative for S100.
21. C. Multiple neurofibromas
with the presence of café au lait and Lisch nodules are consistent with neurofibromatosis
1, associated with mutation of NF1 (neurofibromin). BRAF mutation can be
seen in various disorders, including melanocytic
nevus and melanoma.
Neurofibromatosis
2 has schwannoma,
meningiomas, café au lait, etc, but not Lisch nodules, and is associated with
merlin (NF2) mutation. PDGFB abnormality is associated with dermatofibrosarcoma
protuberans. PTCH mutation is seen basal
cell carcinoma.
22. E. Schwannoma
has cellular
component (Antoni A) that palisades (Verocay bodies), and myxoid component
(Antoni B). Fibrosarcoma
is hypercellular spindle cell neoplasm with a herringbone pattern. Leiomyoma
has cigar shaped nuclei. Meningioma has meningothelial
whorls. Neurofibroma
has slender nuclei. None of these has Antoni A and Antoni B components.
{kind=link}
23. B. Presence of schwannoma and café au lait is
consistent with neurofibromatosis
2, associated with merlin mutation. Also see discussion of question 22.
Back to skin
tumors
Back to contents
Comments
Post a Comment